|
|
Research Papers Indian Pediatrics 2008; 45:653-659 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Efficacy of Two Dose Regimes of Intravenous Immunoglobulin in Rh Hemolytic Disease of Newborn – A Randomized Controlled Trial |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
From the Division of Neonatology, Department of Pediatrics, WHO Collaborating Centre for Training and Research in Newborn Care, All India Institute of Medical Sciences, New Delhi 110 029, India. Correspondence to: Dr Ashok K Deorari, Professor,
Division of Neonatology, Department of Pediatrics, WHO Collaborating
Centre for Training and Research in Newborn Care, All India Institute of
Medical Sciences,
Introduction The use of anti-D prophylaxis in Rhesus negative women has led to a marked decline in rhesus sensitization and hemolytic disease of the newborn. However, sensitization can occur despite anti-D immunoglobulin, particularly if it is given too late or in insufficient dose after a large feto-maternal hemorrhage. Many patients in developing countries do not receive Rh prophylaxis due to inadequate antenatal care or inability to afford anti-D immunoglobulin(1). Hence, Rh isoimmunization resulting in hemolytic jaundice is still a common problem in developing countries. Intravenous immunoglobulin (IVIg) has emerged as an important component of treatment in isoimmune hemolytic jaundice. Use of IVIg has been found to be associated with reduced need of exchange blood transfusion (EBT) in both Rh and ABO isoimmunized neonates(2-5). American Academy of Pediatrics (AAP) recommends the use of IVIg in a dose of 0.5-1.0g/kg in neonates with isoimmune hemolytic anemia(6). However, no consistent effect of IVIg on duration of phototherapy has been seen in prior studies (2-5). One retrospective study has noted a trend towards prolonged requirement of phototherapy in babies receiving the IVIg(7). The difference in results may be due to differences in dose regime of IVIg used in these studies. Till date, only one study has compared two different dose regimes of IVIg viz., single dose versus three doses of 0.5g/kg each(8). We conducted this study to compare the effect of two different doses of IVIg on duration of phototherapy in Rh hemolytic disease. We hypothesized that IVIg, given as soon as possible after birth in a single dose of 1 g/kg compared to a single dose of 0.5 g/kg to a Rh isoimmunized neonates of ³32 week gestation, would reduce the duration of phototherapy at least by 24 hours. Methods This randomized clinical trial was conducted from January 2005 to July 2006 at a tertiary-care hospital. Babies of ³32 week gestational age with Rh positive blood group born to Rh negative mother and having positive Direct Coomb’s test (DCT) were included in the study. Babies with major congenital malfor-mations were excluded. The primary outcome of the study was duration of phototherapy. The secondary outcomes included number of EBTs needed after administration of IVIg, number of packed RBC transfusion needed in these neonates in first 6 weeks of life and duration of hospitalization. With an expected mean difference in duration of phototherapy of 24 h, a error of 0.05, power of 80% and with standard deviation of 24 h the required sample size was 17 babies per group. Assuming a mortality of 10%, the sample size was kept at 19 babies per group. A stratified fixed-block randomization was done with a block size of 6. The babies were stratified by the need of exchange transfusion by the age of two hours. The random number table was generated from an online website(9). Random treatment assignments were placed in serially numbered, opaque and sealed envelopes. The principal investigator and data analyzers were blinded about the allocation of the treatment groups. However, the clinical team managing the cases was aware of the randomization group. The blood grouping of all mothers was done in antenatal clinic. Indirect Coomb’s test was done in all Rh-negative mothers. The antenatal management of these pregnancies was carried out by Department of Obstetrics and included amniocentesis, measurement of peak blood flow velocity in middle cerebral artery and intrauterine transfusions when indicated. The gestational age (GA) of the neonate was calculated from last menstrual period (LMP). If LMP was not known, then first trimester ultrasound date was taken for GA assessment. In the absence of first trimester ultrasound, GA was assessed after birth by Expanded New Ballard Score(10). Soon after delivery of the baby, cord arterial blood sample for hematocrit, blood grouping and Rh typing, DCT and total serum bilirubin (TSB) estimation was collected. If cord blood was not collected for any reason, then baby’s venous blood sample was taken in first 30 minutes of life. At 2 h of age, TSB levels were re-estimated and decision about need for EBT was made (Table I). If EBT was not needed, then these babies were randomized and given IVIg as per intervention regimen. If EBT was needed, these babies were subjected to EBT and then randomized using a different randomization table. IVIg was administered soon after EBT according to inter-vention group. As per our unit policy, all babies received phenobarbitone in a dose of 10 mg/kg on day1 followed by dose of 5 mg/kg/day for next 4 days(11). All babies received breast milk initiated as soon as the neonatal condition allowed. The IVIg was given as an infusion over two hours using infusion pump. During the entire duration of infusion baby was monitored for any adverse drug reaction. TABLE I Baseline Characteristics of the Enrolled Cases*
* All numerical variables are expressed as mean ± SD and categorical variables as number of babies (percent) unless otherwise specified; † Value expressed as median (inter-quartile range). The TSB was estimated every 8±2 hrly in enrolled neonates until 24 h after cessation of phototherapy; then as decided clinically. The TSB measurements were done by twin beam micro-bilimeter (Ginevri Technologie Biomediche, Italy). The criteria for EBT and phototherapy were defined (Table II). Phototherapy was provided with two units of special blue light phototherapy units applied as closely as possible and a fibreoptic blanket on the undersurface of the baby. The total duration of phototherapy in hours was noted. Brief periods of discontinuation of phototherapy for feeding the baby or changing nappy were not excluded while calculating total duration of phototherapy. If a baby required phototherapy again, then the subsequent phototherapy duration was also noted and added to total duration of phototherapy. Table II Clinical Definitions, Procedures and Criteria
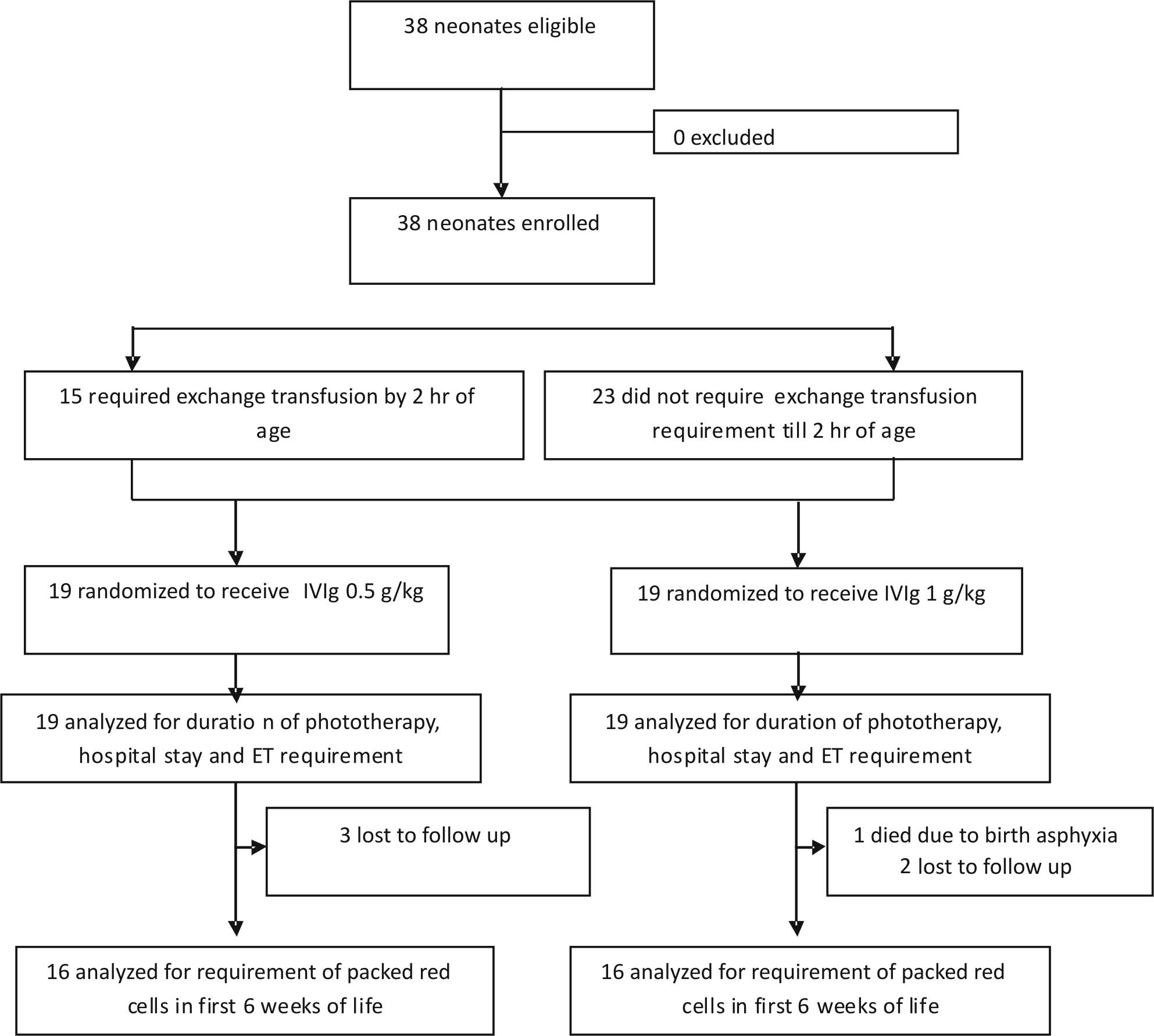
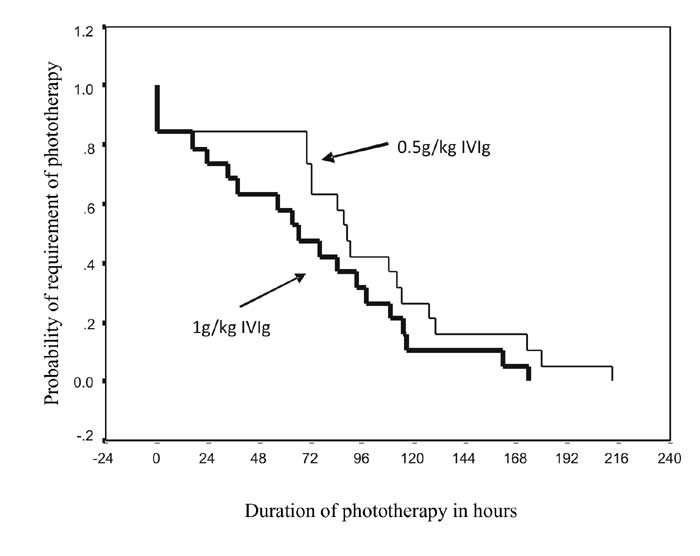
The total duration of hospital stay was also recorded. These neonates were followed up once in two weeks until 6 weeks of life. During this period, infant was monitored for clinical features of anemia. Hematocrit was estimated at 2, 4 and 6 weeks of age. Packed RBC transfusion was given if criteria for transfusion were met at any time during hospital stay or follow-up. Informed consent from at least one of the parents was taken for enrollment in the study. The study was approved by the Ethics Committee of the Institute. Statistical analysis: Patient information was collected in a pre-designed performa. Data entry and analysis were done using Epi-info version 6 software. Continuous data with normal distribution was analyzed by Student’s t-test and non-normally distributed data by Mann Whitney U test. Categorical data were analyzed by Fisher exact test and Chi-square test. P value of <0.05 was taken as significant. Kaplan Meir survival plot was used to compare duration of phototherapy in the two groups. Results During the study period, a total of 38 neonates fulfilling the inclusion criteria were born and all these cases were enrolled in the study (Fig. 1). The baseline maternal and neonatal characteristics of both the groups are given in Table I. Table III provides the summary of different study outcomes. Data on other variables measured in this study are also given in the same table. No difference in duration of phototherapy was noted between the two groups. There was no significant difference even after adjusting for hydropic status of neonates at birth and intrauterine transfusions. At any given time, a similar proportion of neonates in the two groups were being treated with phototherapy (Fig. 2).
Table III Effect of 0.5g/kg vs. 1.0g/kg of IVIg on Outcome Variables
*Data expressed as mean ± SD, †Data expressed as absolute number of events, ‡ n=16 in both groups
Of the 38 enrolled cases one case in 1g/kg group died during hospital stay. That baby had severe birth asphyxia with poor respiratory efforts and died on day 9 of life. Five other babies (3 in 0.5g/kg group and 2 in 1g/kg group) were lost to follow-up. Hence data on packed RBC requirement and packed cell volume at 6 weeks of life was available in only 32 babies. 15 of these 32 babies needed 24 transfusions during their first 6 weeks of life. Eight babies in 0.5g/kg of IVIg group required 12 transfusions while 7 babies of 1g/kg of IVIg required 12 transfusions. Subgroup analysis based on hydropic status at birth, requirement of intrauterine transfusions and by requirement of EBT prior to randomization did not show any significant difference between the two dose regimes. Discussion In this randomized controlled trial, we have compared 0.5g/kg and 1.0g/kg dose regimens of IVIg in Rh-isoimmunized neonates and have observed a comparable duration of phototherapy in the two groups. Peak serum bilirubin and need of EBT were similar in the two groups. Lowest PCV, PCV at 6 weeks and number of packed red blood cell transfusions were also comparable. Although the difference did not reach statistical significance, neonates in high dose group were more likely to be hydropic or having received intrauterine transfusion than neonates in low dose group. Even after adjusting for these two confounding variables and on doing subgroup analysis based on presence of hydrops, duration of phototherapy in the two groups remained comparable. Despite inequality in illness severity (presence of hydrops), comparable proportion of neonates needed EBT in high and low dose groups. This may be due to aggressive antenatal management of hydropic babies with intrauterine transfusions which is known to decrease the need of EBT after birth. Our study has certain strengths and limitations. Although, at least five randomized controlled trials have been conducted till date over the role of IVIg in hemolytic hyperbilirubinemia in neonates(3-5,8,12), the comparative effect of dose of IVIg on duration of phototherapy has been inconclusive. To the best of our knowledge, this is the first randomized controlled trial comparing two different dose regimens of IVIg with an adequate sample size and follow-up for late-onset anemia. As need of EBT and duration of phototherapy in Rh-isoimmunized neonates are influenced by antenatal management(13), results of our study may not be generalizable to many hospitals in the developing countries where facilities for intrauterine transfusions are not available. Role of various dose regimens of IVIg in a setting with less severely isoimmunized babies and lack of facilities for invasive intrauterine transfusions needs to be investigated. Although comparable number of packed RBC transfusions were given for correction of anemia in high and low dose groups, one hydropic baby in 1.0g/kg group required 5 packed RBC transfusions due to severe illness and one baby in 0.5g/kg of IVIg group required 2 packed RBC transfusions due to Plasmodium vivax malaria infection. Due to these two cases, it may be difficult to derive conclusions on the need of subsequent packed RBC transfusion from current study alone. Although similar proportion (21%) of neonates in low and high dose groups needed EBT after IVIg therapy, this is higher than the 12-14% reported previously(2-4). This may be due to more severe cases being enrolled in our study. This is the only randomized controlled trial comparing 0.5g/kg versus 1.0g/kg of IVIg. The higher dose could not have had additional benefit possibly because the Fc receptors in the reticuloendothelial system were saturated by the smaller dose. To conclude, this study shows that the cost of therapy can be reduced by administration of a lower dose of 0.5g/kg of IVIg. Contributors: GG had primary responsibility for protocol development, patient screening, enrolment, outcome assessment, preliminary data analysis and writing the manuscript. DC, RA, VKP and AKD participated in the development of the protocol, in supervising enrolment and writing of the manuscript. Funding: Indian Council of Medical Research (ICMR). Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()