|
|
Research Papers Indian Pediatrics 2007; 44:587-591 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
BMI and Body Fat Percent: Affluent Adolescent Girls in Bangalore City |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
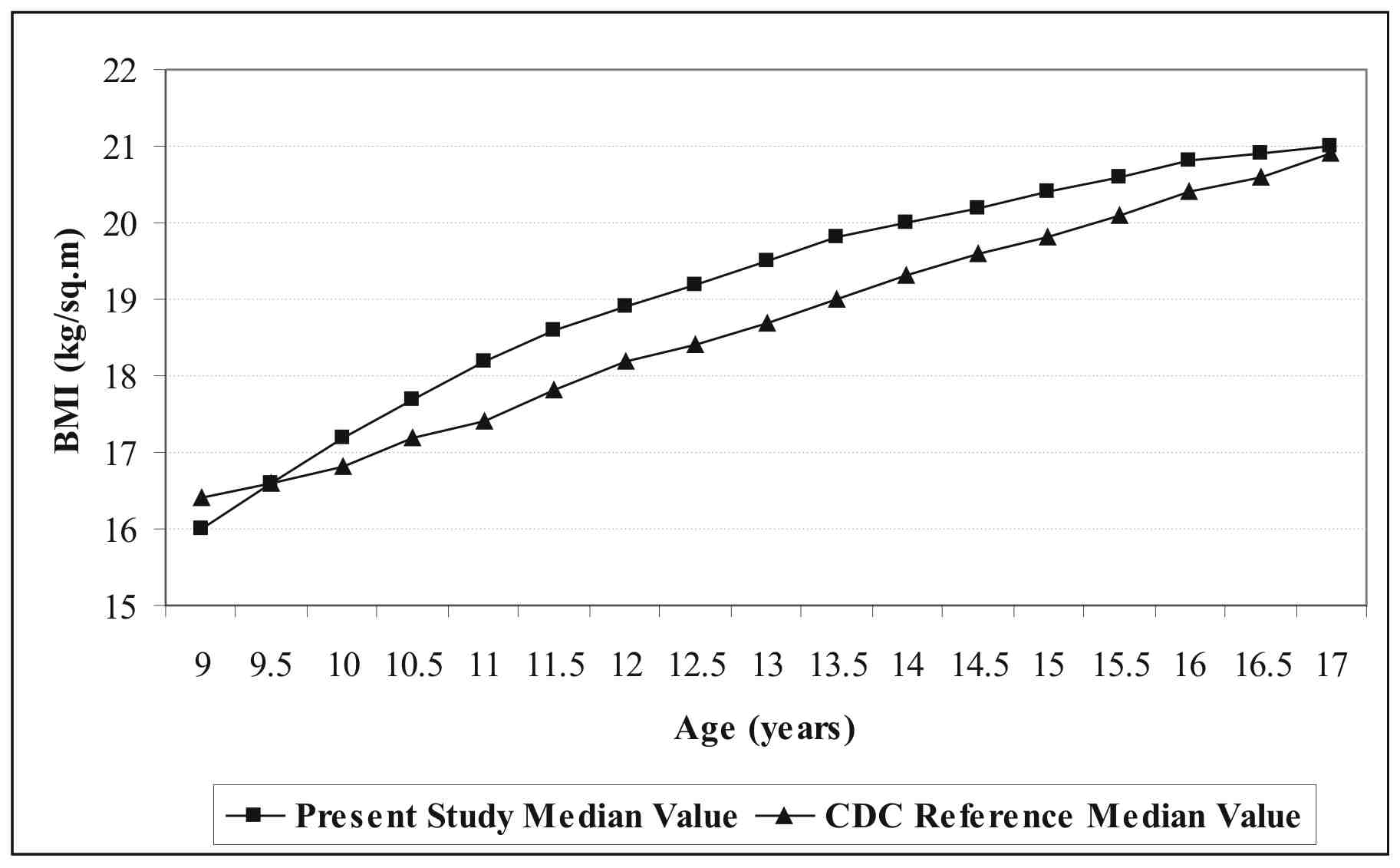
Obesity in childhood is associated with an increased incidence of hypertension, diabetes, coronary artery disease, osteoarthritis and overall increase in morbidity and mortality during adult life(1). There is increasing evidence that children and adolescents of affluent families are overweight; possibly because of decreased physical activities, sedentary lifestyles, altered eating patterns and increased fat content of the diet(1,2). Currently, the body mass index (BMI) is used widely as an indicator of the risk of overweight and of presence of overweight, because of the relative ease and accuracy of the basic measurement(3). However, the BMI has limitations; it tends to have high specificity, but low and variable sensitivity in children and adolescents. Further, the validity of BMI across diverse samples of youth has not been evaluated(4). Limited data is available to assess this nutritional disorder and hence, the present study was conducted to assess the BMI and body fat per cent among the affluent adolescent girls (9-18 years) in Bangalore city and to determine the prevalence of overweight and obesity. Subjects and Methods The study was conducted in a a semi-longitudinal manner at a public school of Bangalore city catering to the affluent society. The subjects were girls between nine and 18 years, attending this school. The consent was taken from the respondents and their families before the initiation of the study. Sampling was done by multistage stratified random sampling procedure. A total of 794 subjects (9 to 18 years) were selected. These girls were categorized in different age categories at an interval of six months. They were studied longitudinally for two and a half years, with data collection every six monthly. The data was collected by a single person. It took 6 months (± days) to complete one round after which the next round of data collection would begin. The subjects at every consecutive reading reached the next level age category, and were crosslinked with the successive age group girls. Due to crosslinking of data, the sample size increased from 794 to observational 3970 girls. The exact age of the children was verified from the school records. A semi-structured pre-tested questionnaire was administered to each child to collect data on socio-demographic profile (age, sex, socio-economic status). Anthropometric measurements (weight and standing height) were taken by standard methodology(5). Weight and fat% was recorded using Tanita body fat monitor/scale TBF-531 with a sensitivity of 0.2 Kg and 0.5% fat. The equipment works on the principle of leg-to-leg Bioelectrical Impedance Analysis (BIA) technique for calculating fat%(6). The results of body fat per cent by BIA technique were validated by comparing with results of BF per cent by standard deuterium dilution method(7) on a sub-sample of 20 girls. The recommended BMI-for-age cut-offs(8) were used for comparing the BMI-for-age of subjects in the present study with the BMI-for-age values of CDC growth charts-2000(9). BMI-for-age was also compared with international cut-off points given by Cole, et al.(10) in 2000 for body mass index for overweight and obesity by sex and age (2-18 years) defined to pass through BMI of 25 and 30 kg/m² at age 18. Statistical Analysis: All results of quantitative parameters were expressed as mean, median, standard deviations and percentiles. The percentiles (5th, 50th, 85th and 95th) were smoothed by the Goldstein method(11). The anthropometric data were analyzed for difference in mean values between two groups within a particular parameter by using Z-test. Correlation between two variables was also done. The results of correlation were regression and were expressed as ‘r’ (the regression coefficient). Results A total of 3970 observational sample represented an initial sample of 794 subjects. Fifty eight percent of the children belonged to nuclear families and 95.7% of the subjects belonged to families with per capita income per month of over Rs. 1,500/-. The mean age of onset of menarche of the girls was 12.01 ± 0.46 years. Table I depicts the mean BMI, mean body fat per cent, velocity with percent change in BMI and body fat percent, and prevalence of obesity and overweight in adolescent girls at 6 monthly age intervals between 9-18 years of age. The age-specific median values for BMI of the affluent adolescent girls in Bangalore, plotted in relation to the 50th percentile of CDC BMI-for-age reference data, are shown in Fig.1. Table I The mean BMI and BMI Velocity in Adolescent Girls (n= 3970)
*Z: Value significant at P <0.05. ** Prevalence rate calculated using international cut-offs given by Cole, et al.(11).
Using the BMI-for-age values–CDC 2000(9) subjects were assessed for underweight, overweight and obesity. About 13.1% of the girls had BMI-for-age between 85th percentile and less than 95th percentile indicating overweight. A little less than 5% of the subjects had values equal to or above 95th percentile indicative of obesity. At the same time 5.1% of the subjects were less than the 5th centile indicating underweight. Table I presents the frequency of subjects in the range of overweight and obesity of BMI-for-age in comparison to international cut-off points given by Cole, et al.(10). The highest prevalence rate of overweight was found in girls at 11.5 years which is around six months before the mean age of menarche of these girls. It was seen that high prevalence of overweight started at around the peak height and weight velocity period (11.0 years) and ended at around the time of culmination of growth spurt period (13.0 years), where the highest prevalence of obesity among the girls was also observed. The body fat percent obtained by deuterium dilution and BIA method, showed a significant high correlation (r = 0.86, P <0.01). The mean systematic bias fat percent was also calculated and it was found that BIA overestimates the body fat percent (–3.66%) (the value of difference is more than the value by deuterium dilution technique). This bias was adjusted in the readings of body fat percent estimated by BIA technique in the study. Table I also shows that the mean body fat percent significantly increased at 11.0 years which was again just a year before the onset of menarche and continued even six months after the mean age of onset of menarche. The smoothed percentile values of body fat per cent of the girls are given to assess normal (50th percentile) to under (5th percentile) to over weight (85th and 95th percentile) to obesity (>95th percentile) as per the criteria given by WHO(8) for BMI (Table II). Table II Smoothed Percentile Values Representing the Body Fat Percent-for-age
Discussion In the present study the prevalence of overweight and obesity in affluent adolescent school girls in Bangalore according to CDC BMI-for-age criteria was found to be 13.1% and 5.0% respectively. A study done in a public school in Delhi also revealed the prevalence of overweight amongst affluent girls as 31%, of which 7.5% were frankly obese(2). In a similar study done amongst affluent adolescent girls (10 to 15 years) of Chennai in 1981 and 1998 the prevalence of overweight and obesity denoted by BMI above 85th and 95th percentile respectively was assessed. It showed that 9.6% of the girls were overweight and 6% were obese(12). Higher velocity of BMI and body fat percent in our study were found during the pubertal period, between 10-12 years. This may be associated with the increase in adipose tissue and overall weight gain during the pubertal growth spurt(13). Stage of sexual maturation may be a confounder when interpreting BMI as an indicator of the risk of overweight and of presence of overweight. On an average, BMI increases with the stage of sexual maturation in girls, but the estimates of relative fatness are variable, especially in girls who have just attained menarche(14). To overcome the variable sensitivity in children and adolescents, BMI could be clubbed with actual measures of fatness rather than the use of BMI alone. We thus, recommend that future studies of body fat (‘adiposity’) in Indian children and adolescents should be formulated rather than rely solely on BMI cut-points of obesity. The percentile values estimated from the present study could be used as the base line data for the formulation of the standards for these girls. Also, further work is required to compare the usefulness of percent BF cutoffs with that of BMI classifications of overweight and obesity in predicting increased metabolic risk in children and adolescents of all ages and ethnicities. Acknowledgements We thank Dr. Stella Samuel, Principal, Bishop Cotton Girls High School, St. Marks Road, Bangalore, for the help extended during the study. We would like to thank Ms. Vanija Samuel and Mr. Solomon, teachers and students for their kind co-operation in the data collection. We also extend our thanks to Dr. Justin V Gnanou, Lecturer, Department of Biochemistry, St. John’s Medical College, Bangalore and all the paramedical staff members for their help in conducting the validation study. Contributors: AS, PS and SS were involved in designing the study. AS did the data collection along with AVK and SM. AS, AVK and SM involved in analyzing the data. All were involved in preparation of the manuscript. Dr. Sood will stand guarantee to the study. Funding : None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()