|
|
Images in Clinical Practice Indian Pediatrics 2005;42:829-830 |
||||
|
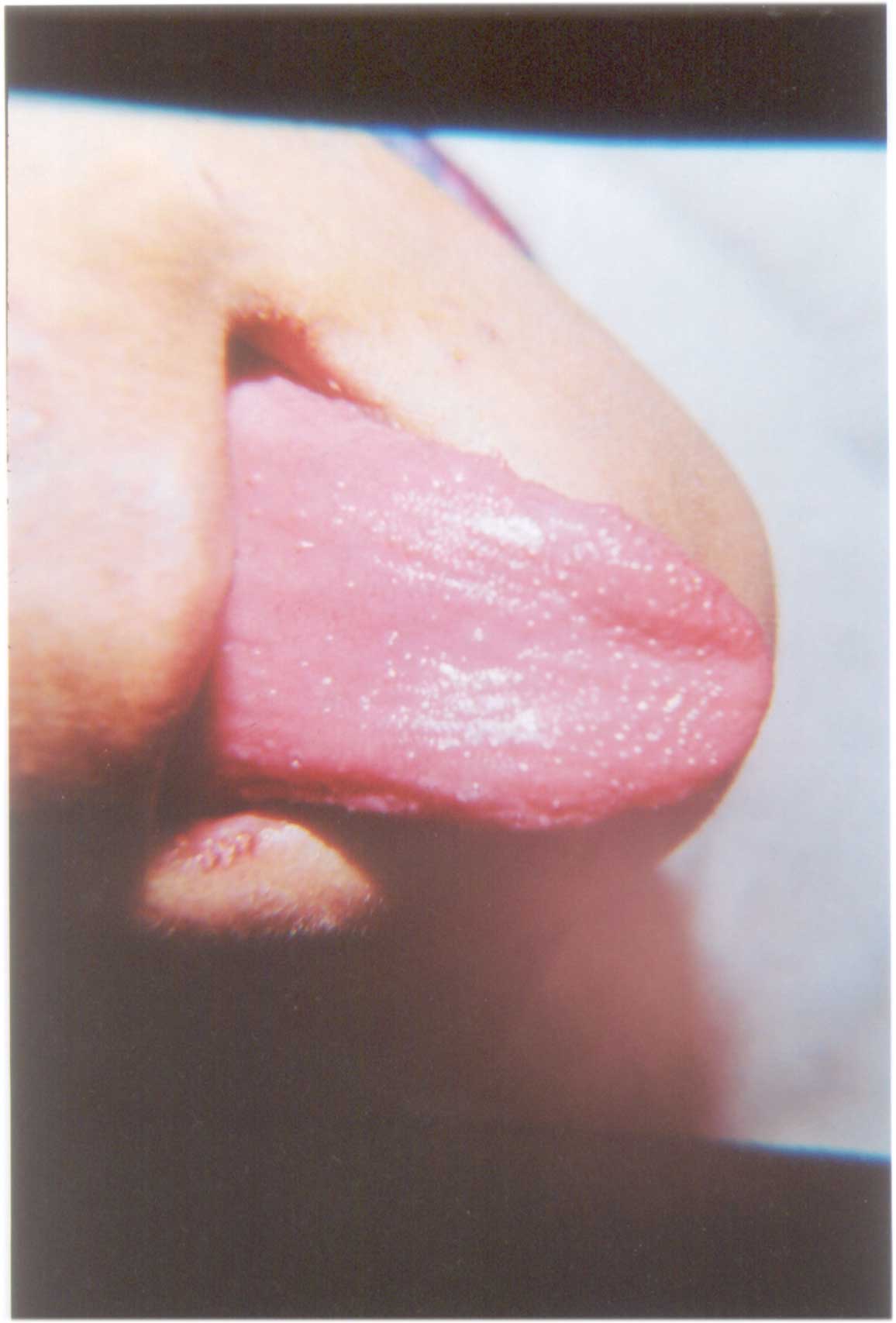
Scarlet Fever |
||||
|
Scarlet fever is an acute exanthem caused by any of the three exotoxin (erythrotoxin) producing but antigenically unrelated hemolytic strains, types A, B or C, Streptococci. Depending upon the previously acquired antitoxic immunity, the patient will develop either scarlet fever, or tonsillitis or cellulitis. Upper respiratory tract is the usual portal of entry. The disease is endemic world over but the full syndrome is uncommon in tropics where sub clinical infection is frequent. Most cases occur between 1-10 years of age and may occasionally be seen in adults. Initially the tongue has heavy white coating and red swollen papillae appear 2-3 days later giving it a "white strawberry tongue" appearance. By 4-5th day, as the coating is shed, the tongue becomes smooth, bright red, has prominent papillae and appear as "red strawberry tongue" before reverting back to normal. By 2nd day a fine popular, punctate erythematous skin rash, that gives sand paper feel, begins in cephalo-caudal fashion. Accentuation of skin creases with transverse red streaks or Pastia’s lines are seen over axillary or antecubital folds. Complications may occur either due to streptococcal toxin (myocardits), or bacterial invasion (septic arthritis, meningitis, osteomyelitis) or by an allergic reaction (rheumatic fever, glomerulonephritis). White coated tongue in oral thrush or suburral tongue that occurs due to decreased salivary flow or tongue movements as in mouth breathers, or soft food eaters; and beefy red edematous tongue seen in early pellagra may some times be confused with strawberry tongue of scarlet fever but can be clinically differentiated without much difficulty. Kawasaki’s disease having features of lingual erythema with prominence of papillae and resembling strawberry tongue, generalized scarlatiniform eruptions, cervical lymph-adenopathy and acute febrile illness closely mimics scarlet fever. However, high clinical suspicion, characteristic eventuation of strawberry tongue, culture of Streptococci from pharynx, surgical wounds or cellulitis and a rising ASO titre are diagnostic and will also exclude staphylococcal scarlatina, viral exanthem and drug rash. Though a single episode of scarlet fever will confer permanent antitoxin immunity, the recurrences are not unusual. This is due the fact that toxin produced by other strains is not neutralized and the bacterial immunity is temporary. Early treatment with penicillin (alternatively erythromycin) could help in prevention of complications. Vikram K. Mahajan,
|
![]()