|
|
Personal Practice Indian Pediatrics 2004; 41:787-795 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Anil Vasudevan
Nephrotic syndrome, characterized by heavy proteinuria and hypoalbuminemia, is an important chronic disorder in children. Edema is the chief clinical manifestation, which may vary from mild periorbital puffiness to anasarca. In most patients, the edema is mild and transient, and resolves following therapy with corticosteroids (steroid sensitive nephrotic syndrome) alone. The management of edema is, however, cumbersome in those with severe relapses and in those with resistance to corticosteroid therapy. Treatment with diuretics is indicated in patients with significant edema or symptomatic fluid overload. Intravenous infusions of albumin may be required in certain situations. Current concepts on the pathogenesis and management of edema are reviewed in this article. Pathophysiology of Formation of Edema Fluid movement across capillaries is normally the result of a balance between filtration and reabsorption due to changes in capillary and tissue hydrostatic and oncotic pressures. Any disturbance in this balance, favoring increased filtration and/or decreased reabsorption results in edema. While the pathogenesis of edema in nephrotic syndrome is not well understood, it is usually attributed to an expansion of the interstitial compartment secondary to increased fluid transfer across capillary walls, or accumulation of sodium secondary to an intrarenal defect. Major sites involved in edema formation are (i) capillaries - where there is disruption of Starling equilibria, and (ii) the kidney - where there is primary salt retention. According to the classical view, vascular underfill is responsible for the formation of edema(1,2). Proteinuria results in hypoalbuminemia and lowers plasma oncotic pressure. This alters Starling forces, determining the distribution of fluid between plasma and interstitium, and results in an increase in interstitial fluid and edema. The resultant hypovolemia activates the reninangiotensin-aldosterone axis, the sympathetic nervous system and vasopressin secretion leading to renal salt and water retention, which further aggravates the edema. However, a normal plasma volume, and normal blood levels of renin and aldosterone in some patients with nephrotic syndrome does not support this mechanism(3,4). According to the overfill hypothesis a primary intrarenal defect in sodium handling is responsible for the occurrence of edema(5). This results in decreased filtration per nephron, increased tubular reabsorption, and decreased sensitivity to atrial natriuretic peptide, leading to fluid retention. Studies in animals with experimentally induced nephrotic syndrome, suggest that stimulation of tubular sodium reabsorption occurs in the collecting duct(6). Resistance to the action of atrial natriuretic peptide, due to enhanced activity of cyclic-GMP phosphodiesterase and increased activity of Na+-K+ ATPase might contribute to increased tubular sodium resorption. Finally, the human body is equipped with defense mechanisms that limit excessive capillary fluid filtration. These mechanisms include increased interstitial hydrostatic pressure and lymph flow, decreased interstitial oncotic pressure and reduced permeability of the capillaries to proteins. Edema results when these adaptive mechanisms are inadequate(7). It is suggested that while vascular underfill is responsible for most cases of edema in minimal change disease, other mechanisms might be important in patients with non-minimal disease. There is increasing evidence that hypoalbuminemia and the inability of the renal distal tubule to excrete sodium are not the only factors responsible for the occurrence of edema. Increased vascular capillary permeability, related to the release of vascular permeability factor and other cytokines, may also play an important role in the pathophysiology of nephrotic edema(8). Management of Edema Therapy for edema is necessary since fluid retention predisposes to infections and can exacerbate preexisting hypertension. Anasarca with ascites and pleural effusions may cause respiratory embarrassment. Edema of intestinal walls may result in diarrhea. Children with edema have restricted activity and low self-esteem. Assessment of Fluid Status Determination of fluid status is important in the initial evaluation. Assessment of intravascular volume is achieved by clinical and biochemical features, and radiological investigations. Hypovolemia is characterized by tachycardia, low normal or low blood pressure, features of dehydration and elevated blood levels of urea disproportionate to creatinine. Measurement of urinary concentration and fractional excretion of sodium (FENa) assist in the evaluation of fluid status. The normal urinary sodium concentration varies between 30-40 mEq/L; values below 20 mEq/L indicate sodium-conserving states, e.g., hypovolemia, dehydration and pre-renal ARF. FENa (percent), the ratio of sodium excreted to that filtered by the renal tubules, is below 1% in sodium retaining conditions.
(urinary Na+) × (serum creatinine) × 100 The ratio of urinary concentrations of K+ to the sum of K+ and Na+ (urinary K+/ K+ + Na+) is also a satisfactory index of activation of the reninangiotensin-aldosterone axis(9). A ratio of more than 0.6 or 60% suggests activation of the axis and renal potassium wasting. Patients with nephrotic syndrome and hypovolemia typically show low FENa (often below 0.2%) and high urinary K+/K+ + Na+ (ratio greater than 60%)(9). Such patients should not receive oral or intravenous diuretics, before correction of their intravascular volume with either crystalloids or colloids. Patients with edema and no clinical or laboratory features of hypovolemia (normal levels of blood urea, FENa >1% and urinary K+/ K+ + Na+ <60%) can safely be treated with potent diuretics. It is however important to understand sodium wasting due to prior therapy with diuretics often limits the practical utility of these indices. A number of radiological investigations are proposed to be useful for assessing fluid status in patients with nephrotic syndrome. Determination of the diameters of left atrium and inferior vena cava and their change with respiration, on ultrasonography, may provide an accurate assessment of intravascular volume(10). The precise role of these measurements in the management of patients is however not defined. In steroid responsive nephrotic syndrome, treatment with daily corticosteroids usually leads to diuresis within 7-10 days. Treatment for minimal periorbital puffiness or pedal edema is therefore not required. Patients showing moderate to severe edema need specific treatment for its control (Table I). Most such patients show reduction of edema with modest restriction of sodium intake and oral administration of frusemide. Aggressive therapy for edema is required in less than 10% patients. TABLE I Measures for Control of Edema
Sodium Restriction The recommended dietary allowance for calories and protein, appropriate for that age, should be ensured. No restriction on intake of salt and water is necessary in most subjects. Patients with edema should consume unprocessed foods like vegetables, fruit, fish, chicken and meat, all of which contain small amounts of salt. Use of table salt and items with high sodium content should be avoided. Sodium content of some common foods is listed in Table II. The replacement of common salt by low sodium salts (e.g., LONA) is not recommended. TABLE II Sodium Content of Common Foods
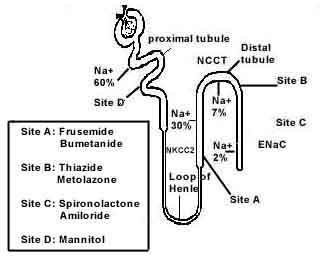
1 mEq of Na+ = 23 mg Na+ or 58.3 mg common salt. Strict salt restriction, limiting sodium intake to 1-2 mEq/kg/day is necessary only in subjects with refractory edema (see below). Diuretic Therapy Diuretics, the standard therapy for edema, act by increasing urinary sodium excretion. Based on their site of action on the renal tubule they are classified as highly potent loop diuretics, moderately efficacious thiazide diuretics, potassium sparing diuretics, osmotic agents like mannitol and carbonic anhydrase inhibitors (Fig. 1).
Factors affecting response to diuretics (a) Potency of diuretics is chiefly determined by its site of action in the nephron (Fig. 1). Most filtered sodium is reabsorbed in the proximal tubule (55-60%) and loop of Henle (25-30%). However, the efficacy of proximally acting diuretics (e.g., acetazolamide) is offset by compensatory increased distal resorption of sodium and water in the ascending limb of Henle. Loop diuretics, on the other hand, can increase FENa to 30%, thiazides to 5-10% and potassium sparing diuretics to 2-3%. (b) Dose response curve defines the intrinsic potency of a diuretic and is generally sigmoid shaped. While administering loop diuretics, it is important to ensure that each dose reaches the steep part of the dose response curve before the dose frequency is adjusted. For example, a patient who does not respond to 20 mg of frusemide may not be attaining adequate tissue levels. The single dose should be increased to 40-60 mg rather than giving the same doses twice a day. Using diuretics in two or three daily doses is rational only if each dose exceeds the diuretic threshold. (c) Bioavailability varies widely between different loop diuretics (50% for frusemide, 80% for torasemide, 90% for bumetanide)(11). Limited bioavailability can usually be overcome by appropriate dosing. (d) Drug delivery to its active site is also an important factor. Most diuretics act on the luminal surface of the renal tubule, reaching the tubular lumen by an organic anion secretory pathway in proximal tubules. Loop diuretics are highly bound to proteins, which limit them to the vascular space. Marked hypoalbuminemia thus results in entry of the diuretic into the interstitial space and thereby slower secretion into the tubules. Renal failure results in impaired diuretic excretion, in part because of retention of organic anions (e.g., hippurate) that compete for secretion by the anion secretory pump. Finally, free drug that is secreted into tubular lumen may be bound to filtered intratubular albumin, rendering the former inactive. In experimental models, nephrotic range albuminuria is found to diminish the response to intraluminal frusemide by as much as 50%(12). Medications and strategy Several therapeutic strategies are employed depending on the severity of edema. When starting therapy, it is important to establish a goal, usually a weight loss of 1% body weight daily. While frusemide is used most commonly, additional therapy with a thiazide diuretic is indicated in certain instances. Potassium sparing diuretics, most often spironolactone, are administered chiefly to prevent diuretic-induced hypokalemia. Loop diuretics: The site of action of frusemide, bumetanide and torasemide is at the thick ascending loop of Henle, where they inhibit the action of the NKCC2 cotransporter (Fig. 1), resulting in sodium, potassium and chloride wasting with diuresis. Frusemide is available for both oral and parenteral administration. Its onset of action is rapid, usually within 30 minutes after oral and 5 minutes after intravenous administration. Oral administration results in peak diuresis at 2 hr, with duration of action of 6-8 hr. The dosage can be increased until maximum recommended doses are reached (Table III). Oral dosing is preferred due to more sustained diuresis. Oral frusemide absorption is slower than its clearance leading to ‘absorption-limited’ kinetics. Effective frusemide concentrations in the blood, there-fore, persist longer when the drug is given by mouth, because of the reservoir in gastro-intestinal tract. TABLE III Dosage of Diuretics
* Metenix (Borg, Zydus Cadila) 5 mg. **Esidrex (Novartis) 50 mg; Aquazide (Sun Pharma) 25 mg; Biduret-L (Glaxo) 25 mg with amiloride 2.5 mg. Intravenous administration of frusemide, either as bolus or infusion, is preferred in patients with intractable edema and/or reduced glomerular filtration rate. Intravenous boluses are given slowly over 10-15 minutes (not exceeding a rate of 4 mg/min) to minimize the risk of ototoxicity and autonomic symptoms like weakness, dizziness, nausea and vomiting. Intravenous bolus therapy is however, associated with periods of both supramaximal and submaximal excretion, resulting in part of the medication being secreted ineffectively into renal tubules. Continuous infusions of frusemide are safer and more effective than intravenous bolus injections in subjects with refractory edema. A continuous infusion maintains a constant rate of drug secretion into the renal tubules. The chief indication for its use is in hospitalized patients with marked edema who show a diuretic response to an intravenous bolus, which is not sustained. Patients who show no response, to intravenous bolus are unlikely to respond to an infusion since the former achieves higher plasma frusemide levels. After an initial bolus of 1-2 mg/kg, frusemide infusion is started at 0.1 mg/kg per hr and can be increased to 1 mg/kg per hr. The risks associated with high doses of intravenous frusemide, especially hypovolemia and dyselectrolytemia should be weighed against alternative strategies such as addition of a thiazide diuretic or infusion of albumin. Thiazides: Chlorthiazide, hydrochlorthiazide and metolazone act at the distal convoluted tubule where they block the NCCT cotransporter (Fig. 1). Metolazone also has an effect on the proximal tubule, and hence is more potent than other thiazides. The onset of action is within one hr, peaks in 4-6 hr and lasts for 12 hr. Potassium sparing diuretics: Spironolactone, triamterene and amiloride block aldosterone induced stimulation of protein synthesis necessary for sodium reabsorption and potassium secretion. These medications are administered orally and have a delayed onset of action, often as long as 3-4 days. Other diuretics: Mannitol, an osmotic agent can also produce diuresis but the effect is transient. Carbonic anhydrase inhibitors (acetazolamide) have mild diuretic action and are ineffective for management of edema. Complications Physicians should be aware of complications of diuretic therapy including volume depletion, azotemia, hyponatremia, hypokalemia and metabolic alkalosis. Prolonged treatment with thiazide diuretics may result in hyperuricemia and hypomagnesemia. Since potassium-sparing diuretics are rarely used alone, hyperkalemia is uncommon. Use of diuretics must be avoided in patients with diarrhea and/or persistent vomiting. Refractory Edema Edema is considered refractory if therapy with loop diuretics at near maximum doses fails to result in diuresis. Various causes of refractory edema and their management are listed in Table IV. TABLE IV Management of Refractory Edema
Synergistic therapy: Patients who fail to show diuresis despite 48 hr of treatment with an adequate dose of frusemide (or another loop diuretic) might benefit from its combination with thiazides. Hydrochlorthiazide or metolazone has been used frequently in combination with frusemide or bumetanide with similar results(13). When a thiazide is combined with a loop diuretic, the former is best given one hr before the latter. This allows solute transport in the distal tubule to be blocked fully before it floods with solute from the loop of Henle, ensuring sustained and effective diuresis. Rapid diuresis can occur with synergistic therapy, resulting in hypovolemia and hypokalemia. Careful monitoring is required in such situations. Potassium sparing diuretics are used to counteract aldosterone-mediated sodium reabsorption and prevent hypokalemia. Albumin infusion: It is necessary to appreciate the two clinical situations where therapy with intravenous albumin might be useful. Patients with nephrotic syndrome occasionally present with features of hypovolemia, secondary to an acute episode of gastroenteritis or overzealous diuretic therapy. In such instances, the correction of intravascular volume deficit gets precedence over management of edema. Initial replacement of fluids may be achieved using normal saline or 5% albumin at 10-20 ml/kg over 30-60 minutes in such patients. Infusions of hyperoncotic (20%) albumin have also been recommended for treatment of severe hypoalbuminemia and edema. Their usefulness for this indication, either alone or in combination with diuretics is however not proven. Co-administration of albumin and diuretics increases delivery of the latter to the renal tubules, resulting in enhanced sodium excretion(14-16). Although difficult to generate firm conclusions, the combination of 20% albumin and frusemide is likely to provide clinical benefits for selected patients. We recommend that the combination should be restricted to patients who show refractory edema or ascites despite maximized doses of diuretics, and in those with severe hypoalbuminemia. Administration of 20% albumin (at a dose of 1g/kg over 1-4 hr) with frusemide (2 mg/kg) is effective(17). Frusemide may be given as a bolus either midway or at the end of therapy with similar results. Albumin is usually administered as an undiluted solution, but may be diluted with saline or 5% dextrose to increase the infusate volume. The rate of infusion should not exceed 2-3 mL/min for 20% solution. The effect of albumin infusion is transient, with most infusate rapidly lost in urine, unless there is remission of proteinuria. Albumin infusions therefore need to be required repeatedly, usually on alternate days for sustained reduction in edema. Infusion of hyperoncotic albumin carries the risk of aggravating pulmonary edema and congestive heart failure. Therefore, careful monitoring of vital signs and volume status during and after the infusion is recommended. The medication is expensive; the cost of a 100 ml bottle of 20% human albumin is Rs. 2000. Ultrafiltration is a satisfactory method for removing excess fluid in patients with refractory edema and oliguria. Continuous arteriovenous hemofiltration needs an arterial access for removal of blood, its passage through a hemofilter and a venous access for the return. The patient’s blood pressure provides the driving force for hemofiltration. Addition of a blood pump to the system improves ultrafiltration, as in continuous venovenous hemofiltration. Hemofiltration is uncommonly employed in our country due to its costs and lack of expertise. Head out water immersion involves sitting or standing in a tub, immersed up to the neck, for 3-4 hr every day(18). Increased venous return due to hydrostatic pressure results in release of atrial natriuretic peptide, natriuresis and diuresis. While physiologically sound, the technique has limited practical utility. The procedure is cumbersome and requires significant parental cooperation. Restriction of water intake is necessary only in patients with edema refractory to other measures, particularly when associated with reduced urine output. Fluid intake is restricted to insensible fluid losses and urine output in these cases. An algorithm for the management of edema in patients of nephrotic syndrome is given in Fig. 2.
Contributors: AV and MM drafted the paper. AB provided overall framework and concept. He will act as the guarantor of the article. Funding: None. Competing interests: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
1. Glassock RJ, Cohen AH, Adler SG. Primary glomerular disease. In: Brenner BM, Ed. The Kidney, 5th edn. Philadelphia, WB Saunders 1996; pp 1392-1497.
2. Van de Walle JG, Donckerwolcke RA, van Isselt JW, Derkx FHM, Joles JA, Koomans HA. Volume regulation in children with early relapse of minimal change nephrosis with or without hypovolaemic symptoms. Lancet 1995; 346: 148-152.
3. Geers AB, Koomans HA, Boer EJ, Mees Dorhout EJ. Plasma and blood volumes in patients with nephrotic syndrome. Nephron 1984; 38: 170-173.
4. Koomans HA, Geers AB, Mees Dorhout EJ, Kortlandt W. Lowered tissue fluid oncotic pressure protects the blood volume in the nephrotic syndrome. Nephron 1986; 42: 317-322.
5. Schnaper HW, Robson AM. Nephrotic syndrome. In: Schrier RW, Ed. Disease of the Kidney and Urinary Tract, 7th edn. Philadel-phia, Williams Wilkins 2001; pp 1773-1832.
6. Deschenes G, Feraille E, Doucet A. Cellular and molecular mechanisms of sodium pump activation in experimental models of nephrotic syndrome. Nephrologie 2003; 24: 121-126.
7. Van de Walle JG, Donckerwolcke RA. Pathogenesis of edema formation in the nephrotic syndrome. Pediatr Nephrol 2001; 16: 283-293.
8. Brenchley PE. Vascular permeability factors in steroid-sensitive nephrotic syndrome and focal segmental glomerulosclerosis. Nephrol Dial Transplant 2003; 18 (Suppl 6): 21-25.
9. De Santo NG, Pollastro RM, Saviano C, Pascale C, Di Stasio V, Chiricone D, et al. Nephrotic edema. Semin Nephrol 2001; 21: 262-268.
10. Schrier RW, Fassett RG. A critique of the overfill hypothesis of sodium and water retention in the nephrotic syndrome. Kidney Int 1998; 53: 1111-1117.
11. Brater DC. Diuretic therapy. N Eng J Med 1998; 339: 387-395.
12. Kirchner KA, Voelker JR, Brater DC. Intratubular albumin blunts the response to frusemide-A mechanism for diuretic resistance in the nephrotic syndrome. J Pharmacol Exp Ther 1990; 252: 1097-1101.
13. Garin EH. A comparison of combinations of diuretics in nephrotic edema. Am J Dis Child 1987; 141: 769-771.
14. Mees Dorhout EJ. Does it make sense to administer albumin to the patient with nephrotic edema? Nephrol Dial Transplant 1996; 11: 1224-1226.
15. Akcicek F, Yalniz T, Basci A, Ok E, Mees Dorhout EJ. Diuretic effect of frusemide in patients with nephrotic syndrome: Is it potentiated by intravenous albumin? BMJ 1995; 310: 162-164.
16. Elwell RJ, Spencer AP, Eisele G. Combined furosemide and human albumin treatment for diuretic-resistant edema. Ann Pharmacother 2003; 37: 695-700.
17. Fliser D, Zurbruggen I, Mutschler E, Bischoff I, Nussberger J, Franek E, et al. Coadministration of albumin and furosemide in patients with the nephrotic syndrome. Kidney Int 1999; 55: 629-634.
18. Hwang SJ, Tsai JH, Lai YH, Chen JH. Plasma atrial natriuretic peptide and natriuretic res-ponses to water immersion in patients with nephrotic syndrome. Nephron 1991; 58: 330-338.
![]()