|
|
|
Indian Pediatr 2015;52:
335-336 |
 |
Ophelia Syndrome: Hodgkin Lymphoma with Limbic
Encephalitis
|
|
Monica Juneja, Satnam Kaur, Devendra Mishra and
*Silky Jain
From Department of Pediatrics, Maulana Azad Medical
College and associated Lok Nayak hospital; and *Department of Pediatric
Hemato-Oncology, Rajiv Gandhi Cancer Institute and Research Centre,
Rohini; New Delhi, India.
Correspondence to: Dr Satnam Kaur, Assistant
Professor, Department of Pediatrics, Maulana Azad Medical College and
associated Lok Nayak Hospital, New Delhi 110 002, India.
Email: [email protected]
Received: September 8, 2014;
Initial review: October 21, 2014;
Accepted: February 10, 2015.
|
|
Background: Limbic encephalitis, an immune-mediated encephalitis,
results from inflammation in the medial temporal lobes. The
paraneoplastic form is rare in pediatric population, and frequently
precedes tumor diagnosis. Case characteristics: A 9-year-old boy
receiving chemotherapy for Hodgkin lymphoma, developed headache,
temporal lobe seizures, anxiety, hallucinations, short-term memory loss
and autonomic disturbances. Magnetic resonance imaging of brain showed
features suggestive of limbic encephalitis. Electro-encephalography
showed diffuse slowing with no epileptiform discharges. Outcome:
We diagnosed paraneoplastic form of limbic encephalitis. Treatment with
steroids and intravenous immunoglobulin failed, and the child died 4
weeks after onset of symptoms. Message: Limbic encephalitis
should be kept as differential diagnosis in a child with sub-acutely
evolving neuropsychiatric symptoms.
Keywords: Lymphoma, Magnetic resonance
Imaging, Paraneoplastic syndrome.
|
|
Limbic encephalitis is a neurological syndrome
resulting from inflammatory lesions in the medial temporal lobes [1]. It
typically presents with subacute onset of short term memory deficits,
temporal lobe seizures, mood/sleep disturbances and hallucinations, and
may progress to dementia [1]. Paraneoplastic form of limbic encephalitis
is rare in children, but is being increasingly recognized [1]. We report
a child with Hodgkin lymphoma who developed limbic encephalitis while
undergoing chemotherapy.
Case Report
A 9-year-old boy, diagnosed as Hodgkin lymphoma
(mixed cellularity type) three months ago, was admitted for third cycle
of chemotherapy (Adriamycin, Bleomycin, Vinblastine, Dacarbazine). At
admission, he complained of mild, diffuse headache persisting for last
10-12 days. There was no altered sensorium, seizures, focal neurological
deficits or any history suggestive of raised intracranial pressure. The
neurological examination and the fundus evaluation were normal. Two days
later, he developed multiple episodes of complex partial seizures
starting with oromotor sensory symptoms. On the same day, child
complained of difficulty in walking; and on examination was found to
have weakness of the hamstrings on the right side along with bilateral
brisk tendon reflexes and extensor plantar response. Magnetic resonance
imaging (MRI) done on the same day was normal. Cerebrospinal fluid (CSF)
examination showed normal biochemistry, no malignant cells, and negative
herpes simplex virus (HSV) serology. Elecgro-encephaloography (EEG) was
within normal limits. Over the next four days, the child was noted to
have decreased spontaneous activity, overall reduced interaction and
decreased speech. There were long periods of anxiety with insomnia along
with visual hallucinations.
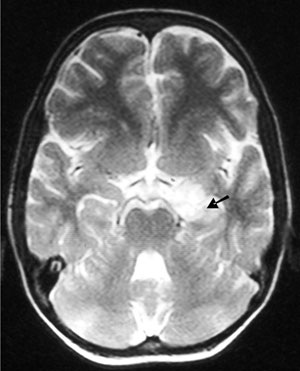
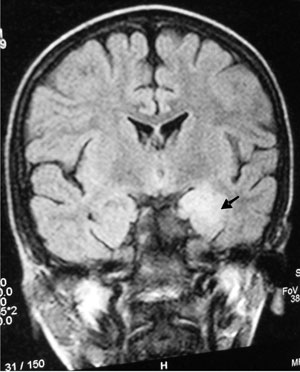
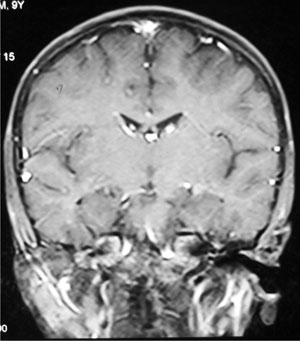
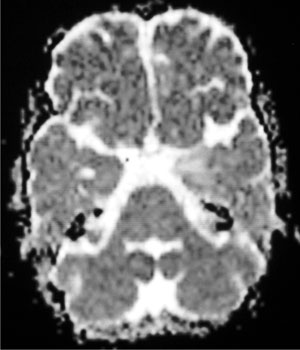
Over next few days, symptoms evolved to short-term
memory loss with intact long-term memory. Repeat MRI showed features
suggestive of limbic encephalitis (Fig. 1). Repeat EEG
showed diffuse slowing with no epileptiform discharges. Repeat CSF study
was normal; examination for oligoclonal bands in CSF could not be done.
Anti-NMDA antibodies in serum were negative. Other neuronal autoantibody
tests, including onconeural antibodies, could not be done. Injection
methylprednisolone (30 mg/kg/day) was started for management of limbic
encephalitis. Subsequently, the child completed a course of intravenous
immunoglobulins (IVIG), but continued to deteriorate with progression of
weakness to all four limbs, cranial nerve involvement, rhythmic movement
disorder involving right upper limb, and autonomic dysfunction. He died
four weeks after the onset of symptoms.
Discussion
Paraneoplastic neurological syndromes are rare
complications of Hodgkin lymphoma [2]. Of all these, cerebellar
degeneration and limbic encephalitis are well-characterized. Association
of limbic encephalitis with Hodgkin lymphoma has also been termed as
Ophelia syndrome. The diagnostic criteria of paraneoplastic limbic
encephalitis formulated by Paraneoplastic Neurological Syndromes
Euronetwork [3] include: (i) subacute onset (days or up to 12
weeks) of seizures, short-term memory loss, confusion and psychiatric
symptoms; (ii) neuropathological or neuroradiological evidence of
involvement of the limbic system; (iii) exclusion of other
possible etiologies of limbic dysfunction; and (iv) demonstration
of a cancer within 5 years of the diagnosis of the neurological disorder
or demonstration of a well-characterized paraneoplastic antibody. The
subacute onset of limbic encephalitis is unlike other neurological
disorders in Hodgkin lymphoma, which are predominantly acute in onset
[4]. Though antibody testing could not be done in our patient, he
fulfilled these criteria. The main differential diagnosis of Herpes
simplex encephalitis was ruled out by negative serology in our case.
The pathogenesis of limbic encephalitis involves an
autoimmune process. It has been broadly categorised into two groups:
associated with antibodies against intracellular neuronal antigens or
with antibodies directed against cell membrane/extracellular antigens
[5,6]. Whereas the first group is frequently associated with cancers
(lung, testis and breast) and responds poorly to treatment, the second
group is less frequently associated with cancers, and responds
favourably to immunotherapy [5-7]. The majority of cases of limbic
encephalitis in children are non-paraneoplastic. In a series of ten
pediatric patients (<18 years) with limbic encephalitis, only one had a
tumour [1]. Our case adds to the few previous reports of paraneoplastic
limbic encephalitis in children [1,8].
Frequently (60%), neurological manifestations of
limbic encephalitis precede tumor diagnosis [8]. In the absence of any
tumor, regular evaluation for tumor occurrence should continue,
especially if onconeural antibodies are detected [1]. Early
immunotherapy is recommened for treatment of limbic encephalitis [9].
Intravenous immunoglobulins, steroids and plasma exchange are usual
first line treatment; cyclophophamide and rituximab are used in
non-responders [6,10].
We conclude that limbic encephalitis should be
suspected in a child with sub-acute onset of psychiatric symptoms, with
or without associated tumor. Initial neuroimaging may be normal and
serial imaging may be required to detect evolving disease.
Contributors: All authors were involved in
patient management, preparation of manuscript, and approving the final
version.
Funding: None; Competing interests: None
stated.
References
1. Haberlandt E, Bast T, Ebner A, Holthausen H, Kluger
G, Kravljanac R, et al. Limbic encephalitis in children and
adolescents. Arch Dis Child. 2011;96:186-91.
2. Graus F, Arin H, Dalmau J. Paraneoplastic
neurological syndromes in Hodgkin and non-Hodgkin lymphomas. Blood.
2014;123,3230-38.
3. Graus F, Delattre JY, Antoine JC, Dalmau J,
Giometto B, Grisold W, et al. Recommended diagnostic criteria for
paraneoplastic neurological syndromes. J Neurol Neurosurg Psychiatry.
2004;75:1135-40.
4. Grimm S, Chamberlain M. Hodgkin’s lymphoma: A
review of neurologic complications. Adv Hematol. 2011;2011: 624578.
5. Tuzun E, Dalmau J. Limbic encephalitis and
variants: Classification, diagnosis and treatment. Neurologist.
2007;13:261-71.
6. Ances BM, Vitaliani R, Taylor RA, Liebeskind DS, Voloschin
A, Houghton DJ, et al. Treatment-responsive limbic encephalitis
identified by neuropil antibodies: MRI and PET correlates. Brain.
2005;128:1764-77.
7. Vincent A, Bien CG, Irani SR, Waters P.
Autoantibodies associated with diseases of the CNS: new developments and
future challenges. Lancet Neurol. 2011;10:759-72.
8. Gultekin SH, Rosenfeld MR, Voltz R, Eichen
J, Posner JB, Dalmau J. Paraneoplastic limbic encephalitis: Neuro-logical
symptoms, immunological findings and tumour association in 50 patients.
Brain. 2000;123:1481-94.
9. Darnell RB, Posner JB. A new cause of limbic
encephalopathy. Brain. 2005;128:1745-6.
10. Lancaster E, Martinez-Hernandez E, Dalmau J.
Encephalitis and antibodies to synaptic and neuronal cell surface
proteins. Neurology. 2011;77:179-89.
|
|
|
 |
|