|
|
Original Article Indian Pediatrics 2005; 42:321-328 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Long-term Outcome in Children with Primary Distal Renal Tubular Acidosis |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
TABLE I Follow-up Details of Individual Patients.
* At diagnosis; † Developed renal failure 2 years after diagnosis; ‡ No improvement in metabolic acidosis despite adequate treatment; M-male, F-female, R-rickets, Fr-fracture, HSDS-Height standard deviation score. TABLE II Height and Weight SDS at Initiation of Treatment and at Last Follow-up.
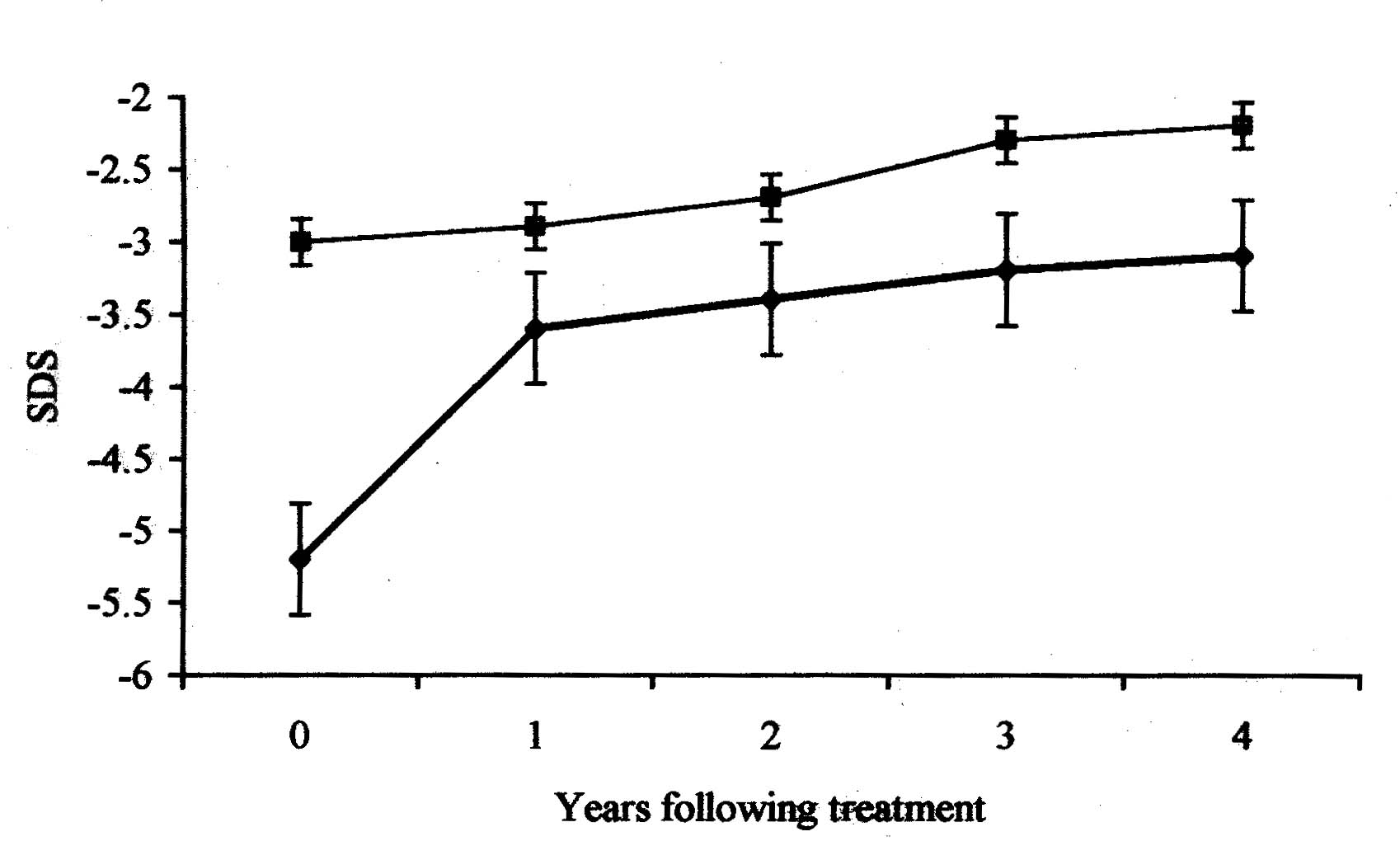
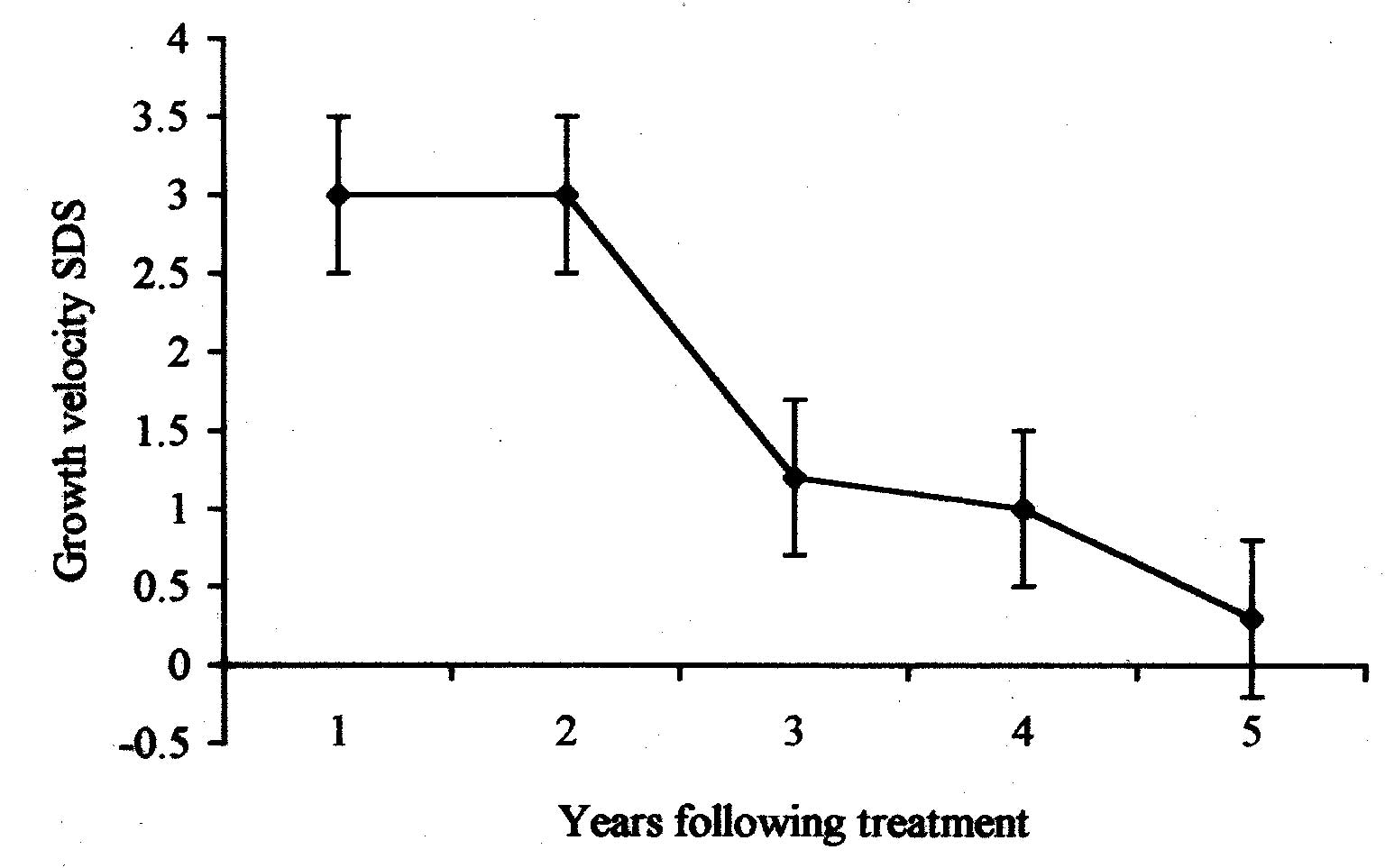
Expressed as median (range), SDS = Standard deviation score. The pattern of height, weight and growth velocity with respect to duration of treatment is shown in Figs. 1 and 2. Growth velocity decreased from 10 cm/yr (4-16 cm/yr) during the first year of treatment to 5 cm/yr (4-6 cm/yr) at four years. This was associated with an increase in height SDS by 1.3 during the first two years of treatment. Height SDS increased by 0.7 during subsequent follow-up.
Factors influencing growth are summarized in Tables III and IV. Height SDS at the end of treatment was not influenced by age at initiation of treatment, follow-up duration, initial height SDS or severity of acidosis at diagnosis. Increase in height SDS correlated negatively with base excess and height SDS on diagnosis and positively with follow-up duration on univariate analyses. On multivariate analysis initial height SDS was the only factor that influenced increase in height SDS. Increase in weight SDS was negatively correlated with base excess and initial weight SDS, with significant association with initial weight SDS on multivariate analyses. A trend of association of age at diagnosis and weight SDS at last follow up was observed (P = 0.07). TABLE III Factors Influencing Height and Weight SDS on Univariate Analyses.
* At the time of diagnosis, r - correlation coefficient, SDS - standard deviation score. TABLE IV Multivariate Analyses for Factors Influencing Height and Weight SDS.
* Regression coefficient provides measure of influence of the
independent variable on the dependent variable. For example increasing
follow-up duration by one year is expected to increase height SDS by
0.1. Bone disease All patients had radiological features of rickets at the time of diagnosis with pathological fractures in four. Serum alkaline phosphatase was normal in 10 patients (62.5%). Radiological findings of rickets resolved in seventeen patients after 4 (1-12) months, without treatment with vitamin D. Nephrocalcinosis Eight patients (44.4%) had radiological evidence of nephrocalcinosis. Twenty-four hour urine calcium excretion was higher in those with nephrocalcinosis than others (P = 0.01); no difference with regards to the age at diagnosis or severity of acidosis was found (Table V). No patient showed renal calcification during follow-up. Five of the 10 patients with hypercalciuria at diagnosis showed reduction in calcium excretion following alkali treatment. Treatment with hydrochlorthiazide was used in the remaining subjects. TABLE V Comparison of Patients with and Without Nephrocalcinosis.
Expressed as median (range). Renal functions Creatinine clearance remained normal in all except one patient. This boy diagnosed at the age of 10 years showed bilateral medullary nephrocalcinosis with normal renal functions at diagnosis. Despite adequate treatment the creatinine clearance declined to 20 mL/min/1.73 m2 2 years later. Discussion The present study shows that appropriate treatment in distal RTA is associated with significant increase in height SDS; final height SDS however remains compromised. There is a paucity of similar published data on growth in children with distal RTA. Rodriguez, et al. (5 patients) and Santos, et al. (24 patients) demonstrated compromised height in children with distal RTA(4, 5). More recently Caldas, et al., showed compromised stature in 28 patients with distal RTA. The mean height SDS was –1.1 for patients diagnosed during infancy and –2 for those diagnosed later(6). The extent of height compromise (final mean height SDS of –2.6) in the present study is greater compared to previous studies. This may be related to delayed diagnosis, greater incidence of bony deformities and lower genetic potential of these patients. An understanding of factors influencing height outcome in subjects with RTA is necessary. In this study, initial height SDS was the only factor that negatively correlated with increase in height SDS. The duration of treatment and severity of acidosis at the time of diagnosis were also found to influence growth on univariate but not on multivariate analysis. This suggests that maximum gain in height SDS was observed in patients who had greatest height compromise at the initiation of treatment. Our findings imply that there is a trend of seeking target height after correction of acidosis. Our failure to demonstrate the effect of age at diagnosis on final height may be related to delayed diagnosis in all the subjects. Majority of our patients were diagnosed after two years of age. It appears that this is a crucial window period for intervention beyond which height is already compromised. These findings are similar to those of Caldas, et al.(6) who observed compromised final height in patients diagnosed after infancy and emphasize the need of early diagnosis and treatment of this condition. Nutritional status influences growth; normal weight for height in majority of our subjects indicates that RTA and not malnutrition was the major factor responsible for growth retardation in our subjects. The pattern of height and growth velocity SDS in our study shows that maximum catch up growth occurs during the first two years of treatment with a decline in growth velocity and increase in height SDS thereafter. Similar findings were demonstrated by others who found that catch up growth was limited to the first two years of treatment(6). This coupled with the fact that increase in height SDS during the first two years of treatment significantly correlated with overall increase in height SDS emphasizes the need for improved management during this crucial period. A high incidence of bony deformities and pathological fractures in this study is distinct from previous reports where rickets was uncommon in children with distal RTA(9). Demonstration of normal levels of vitamin D metabolites and resolution of rickets without treatment with vitamin D suggest a minor role for its altered metabolism in the pathogenesis of bone disease in distal RTA(10,11). It has been suggested that vitamin D status of patients plays a role in determining the extent of bony deformities(6). It is possible that low vitamin D stores in our patients explain the presence of rickets and pathological fractures. A significant proportion of patients with rickets in this study had normal levels of serum alkaline phosphatase. Studies have shown that bone formation is suppressed in patients with distal RTA. Levels of serum alkaline phosphatase, a marker of bone formation, are therefore expected to be normal in these subjects. The incidence of nephrocalcinosis in our study is similar to previous studies(2,6). Prevention of renal calcification is essential for preservation of renal functions in these patients. Hypercalciuria was the only factor that predicted the development of nephro-calcinosis, with no influence of age at diagnosis or severity of acidosis. Our findings emphasize the need for close monitoring and appropriate management of hypercalciuria. While other studies have shown that nephro-calcinosis may develop during treatment(6), we did not find the recurrence in our subjects. Adequate treatment with alkali supplements combined if required, with thiazide diuretics, may thus prevent the development and worsening of nephrocalcinosis. The findings of our study reiterate the need for early diagnosis, appropriate treatment and regular follow-up of patients with distal RTA for improving outcome. Significant height compromise despite adequate treatment emphasizes the need for studies directed at evaluating factors other than metabolic acidosis that are responsible for growth in these patients. Contributiors: MM, PH and AB were involved in management of patients. AnB and AdB planned the study and collected data. AnB performed the literature review and drafted the manuscript. AB designed the study and critically reviewed the manuscript and will act as its guarantor. Competing interest: None. Funding: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()